
Grip, cut, twist, pinch, unbutton, squeeze, wring, prune, chop and type; these 10 things are just the tip of the iceberg when it comes to the huge array of tasks our hands are capable of performing. Unfortunately for many Australians, hand and wrist arthritis can challenge both the ability to use the hands functionally and the capacity to do so without pain.
So, who has hand arthritis?
Whilst there are many diseases (more than 100!) that may cause arthritis of the hand, osteoarthritis is the most common, followed by rheumatoid arthritis. Around 8% of the population has osteoarthritis (self reported); that’s a nearly 2 million Australians! Generally, those affected are older than 45 (the majority are over 65) and close to 2 out of 3 are female. In the US, a study which x-rayed a group (3000+) of community dwelling individuals, found that about 40% of 55-76 year old’s had evidence of hand arthritis (many did not report having arthritis of the hand).
Rheumatoid arthritis, affecting over 400,000 Australians, is the second most common form of arthritis and the hands in this condition are often one of the first areas to experience problems; in fact, the majority of people with rheumatoid arthritis have involvement of the hand and wrist. Again, rheumatoid arthritis is more common amongst females and older age groups.
What is hand arthritis?
By definition, hand arthritis is a condition where there is inflammation of a joint, or joints, of the hand and wrist.
Osteoarthritis has been seen as an essentially degenerative condition (wearing out) rather than an inflammatory condition, but recent research suggests it’s a more varied and complex disorder than this view would suggest. Certainly, some people with osteoarthritis appear to experience more inflammation than others, in the form of tissue inflammation and/or joint effusion (extra fluid in the joint), particularly when they overload the joint (do too much). It is the synovium which lines the capsule, and lubricates and nourishes the joint, that becomes inflamed as part of the immune system’s response to bone and cartilage changes. This in turn contributes to ongoing worsening of the condition.
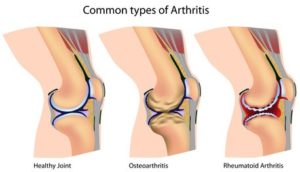
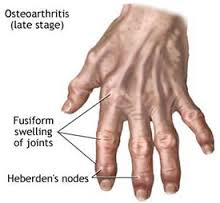
Changes that can be seen on X-ray include joint space narrowing, indicating that the cartilage covering the articulating bones is thinning, osteophytes – little bony growths at the edges of the joint, and increased density of bone in areas deficient in cartilage.
Rheumatoid arthritis is an inflammatory disease that is considered to be an autoimmune condition. Autoimmune means that the body seeks to defend itself against its own tissues, as if that tissue were a foreign body that needed to be destroyed. Although it can affect many parts of the body, synovial tissue (which lines the joint capsule and tendon sheaths) is a special target of rheumatoid arthritis. Synovial tissue proliferation causes local destruction of bone, cartilage, and other soft tissues.
Impact of arthritis
Osteoarthritis often progresses slowly over the course of years, and many people who ‘have’ osteoarthritis are not even aware that they have this condition. Additionally, there is not very good correlation between pain and the severity of osteoarthritis (as seen on X-ray). However, many people with hand osteoarthritis do experience some pain and swelling, and many more will also exhibit stiffness, especially in the morning (usually less than 30 minutes), as well as strength and control deficits, even in the years prior to obvious X-ray changes. This often presents as feeling weak in the hand and struggling with gripping and twisting tasks. Osteoarthritis tends to target the base of the thumb (often the non-dominant hand) and the small joints of the fingers (often the dominant hand).

Rheumatoid arthritis results in significant joint damage as the synovium releases chemicals that break down the bone and cartilage, and the surrounding muscles, ligaments and tendons struggle to stabilise the joint. Rheumatoid arthritis is different for every person but, typically, it is a ‘symmetrical’ arthritis (affects both wrists or both hands) and it is often characterised by episodes (flares) and occasional periods of remission. Pain, warmth, redness and swelling are common symptoms when it is active and it is not uncommon for stiffness to last for an hour or two in the morning, or even longer.
How to manage arthritis
It’s essential to have appropriate early medical management of rheumatoid arthritis. Research is indicating that bone damage happens in the first year or two of disease, so early diagnosis and treatment which may include the use of disease modifying medications (DMARDS), is critical.
Whilst over the counter medications are often used for osteoarthritis, self diagnosis & treatment holds the risk of misdiagnosis, so it’s best to advise your doctor of your issues. According to EULAR (European League Against Rheumatism), osteoarthritis topical treatments such as NSAIDs and capsaicin can be helpful.
The goals of treatment are often quite similar for both osteoarthritis and controlled RA: reduce pain (and swelling), increase grip strength, improve range of motion and improve function. A preventative component is important, particularly in flare ups of rheumatoid arthritis, and involves prevention or limitation of joint damage and minimisation of loss of range, strength and function. The precise strategies to achieve these goals will vary depending on the individual presentation.
What does therapy have to offer?
Conservative interventions for osteoarthritis – including hand exercises, heat, education on joint protection and provision of adaptive equipment and night splints for the thumb – have all been shown to be of benefit. For rheumatoid arthritis, exercises to improve mobility and strength have also shown significant gains in hand function. Splints may also help to reduce pain.
Advice to assist in protecting vulnerable joints (be hand friendly!) from excess load includes suggestions to:
- Use a large grip where possible and avoid heavy lifting – 3 shopping bags in one hand can really add up to a lot of weight;
- Use both hands rather than one, and hold items in a way that shares the load over a number of joints;
- Avoid sustained positions (prolonged grip) or repetitive thumb movements, particularly if the thumb is under load or at extremes of range;
- Use aids to assist where possible – the light shopping trolley vs carrying a basket, jar poppers, electric can openers and more. Lifetec (previously the Independent Living Centre) is a great place to visit to see what’s available.
Exercises shown to be beneficial for arthritis of the hand
As previously stated, an exercise program should be tailored to address the specific deficits and presentation of each individual. It can be said of all the exercises below, that if they are not well tolerated, then modification is required. This list covers some of the key issues of hand arthritis, but isn’t a complete list of all appropriate exercises.
Shoulder and elbow range is likely to be limited in those with rheumatoid arthritis – general shoulder mobility exercises might include reaching behind/overhead, reaching behind the back (this brings both hands toward each other behind your back).
Shoulder/arm strengthening and control (includes postural control) and for the rheumatoid arthritis hand in particular, strengthen the wrist extensor muscles.
Hand mobility work: for the osteoarthritis hand this could be gentle overpressure to straighten the fingers from their flexed position whilst the rheumatoid arthritis hand will more likely benefit from spreading fingers on a flat surface and sliding fingers towards the thumb, as well as doing tendon flexibility exercises. Both groups will benefit from making an ‘O’ between thumb and fingers, to improve thumb mobility.
Hand strength work: the osteoarthritis hand may need to strengthen the muscles at the base of the thumb that lift the thumb away from the hand (extensors and abductors), and working against the resistance of a rubber band around a loose fist can help to achieve this. The rheumatoid arthritis hand will benefit from pinching off hand putty or similar between thumb and index finger, as well as squeezing straight fingers together.
Grip strength is another suitable exercise for both groups – squeezing a tube of hand putty isometrically.
Article courtesy of Carla Mullins,
Pilates studio Director, Trainer & Teacher
Body organics, Brisbane
Oil painting of hands courtesy of Daniel Maidman (creative commons)
References
http://www.niams.nih.gov/health_info/rheumatic_disease/#ra_17
Joint-specific prevalence of osteoarthritis of the hand, Osteoarthritis and Cartilage, September 2006 Vol 14, Issue 9, Pages 953-957. F.V. WilderJ.P. Barrett E.J. Farina
Prevalence of hand symptoms, impairments and activity limitations in rheumatoid arthritis in relation to disease duration. J Rehabil Med. 2010 Nov;42(10):916-21. doi: 10.2340/16501977-0619.Horsten NC1, Ursum J, Roorda LD, van Schaardenburg D, Dekker J, Hoeksma AF.
Goldring SR. The role of bone in OA pathogenesis. Rheumatic Disease Clinics of North America. 2008; 34: 561–571
Rheumatoid Arthritis. Plan to Win. Cheryl Koehn, Taysha Palmer, and John Esdaile (2002)
Zhang W, Doherty M, Leeb BF, et al. EULAR evidence-based recommendations for the diagnosis of hand OA: report of a task force of ESCISIT. Annals of Rheumatic Diseases. 2009; 68:8-17
Valdes K, Marik T. A systematic review of conservative interventions for OA of the hand. Journal of Hand Therapy. 2010; 23: 334–351
Exercises to improve function of the rheumatoid hand (SARAH): a randomised controlled trial. Lancet.2015 Jan 31;385(9966):421-9. doi: 10.1016/S0140-6736(14)60998-3. Epub 2014 Oct 9. Lamb SE, Williamson EM, Heine PJ, Adams J, Dosanjh S, Dritsaki M, Glover MJ, Lord J, McConkey C, Nichols V, Rahman A, Underwood M, Williams MA;Strengthening and Stretching for RA of the Hand Trial (SARAH) Trial Team
A tailored hand exercise program improves function of the rheumatoid hand. J Physiother. 2015 Apr;61(2):96. doi: 10.1016/j.jphys.2015.02.007. Epub 2015 Mar 20. Østerås N, Kjeken I.
EULAR- Evidence based recommendations for the management of hand osteoarthritis. Ann Rheum Dis2007;66:377-388 doi:10.1136/ard.2006.062091
Systematic review of design and effects of splints and exercise programs in hand osteoarthritis . Arthritis Care & Research, Volume 63, Issue 6, pages 834–848, June 2011. Ingvild Kjeken, Geir Smedslund, Rikke H. Moe, Barbara Slatkowsky-Christensen, Till Uhlig and Kåre Birger Hagen
Development of an evidence-based exercise programme for people with hand osteoarthritis. Scandinavian Journal of Occupational Therapy. Volume 22, Issue 2, 2015 pages 103-116.Ingvild Kjeken ab*, Margreth Grotle acd, Kåre Birger Hagenab & Nina Østeråsab
Exercises to improve function of the rheumatoid hand (SARAH): a randomised controlled trial. The Lancet385.9966 (Jan 31, 2015): 421-429. Lamb, Sarah EWilliamson, Esther M; Heine, Peter J; Adams, Jo; Dosanjh, Sukhdeep; et al
The effectiveness of working wrist splints in adults with rheumatoid arthritis: a mixed methods systematic review. Ramsey, Lucia; Winder, Robert John; McVeigh, Joseph G Journal of rehabilitation medicine, 06/2014, Volume 46, Issue 6
Systematic review of design and effects of splints and exercise programs in hand osteoarthritis . Arthritis Care & Research, Volume 63, Issue 6, pages 834–848, June 2011. Ingvild Kjeken, Geir Smedslund, Rikke H. Moe, Barbara Slatkowsky-Christensen, Till Uhlig and Kåre Birger Hagen
Development of an evidence-based exercise programme for people with hand osteoarthritis. Scandinavian Journal of Occupational Therapy. Volume 22, Issue 2, 2015 pages 103-116.Ingvild Kjekenab*, Margreth Grotleacd, Kåre Birger Hagenab &Nina Østeråsab
Exercises to improve function of the rheumatoid hand (SARAH): a randomised controlled trial. The Lancet385.9966 (Jan 31, 2015): 421-429. Lamb, Sarah EWilliamson, Esther M; Heine, Peter J; Adams, Jo; Dosanjh, Sukhdeep; et al
The effectiveness of working wrist splints in adults with rheumatoid arthritis: a mixed methods systematic review. Ramsey, Lucia; Winder, Robert John; McVeigh, Joseph G Journal of rehabilitation medicine, 06/2014, Volume 46, Issue 6
Comments are closed.